Quick Facts
- Prevalence: Approximately 50% to 60% of patients with liver cirrhosis develop esophageal varices.
- Risk Threshold: A hepatic venous pressure gradient of 12 mm Hg or higher is the critical threshold for spontaneous bleeding.
- Size Matters: The one-year risk of a first bleeding episode is roughly 15% for large varices compared to 5% for small ones.
- Urgency: Acute variceal bleeding carries a mortality rate of 10% to 20% within the first six weeks.
- Prevention: Managing portal hypertension through non-selective beta-blockers and lifestyle changes can significantly reduce rupture risk.
- Screening: Regular endoscopy is the gold standard for detecting early warning signs of esophageal variceal bleeding.
Early esophageal varices often present no symptoms until they bleed. Warning signs of a rupture or critical stage include hematemesis (vomiting blood), melena (dark, tarry stools), and lightheadedness due to blood loss. Patients with cirrhosis should also monitor for signs of worsening portal hypertension, such as jaundice, easy bruising, and an enlarged abdomen caused by ascites, which indicate an increased risk of variceal development.
The Root Cause: Portal Hypertension and Esophageal Varices
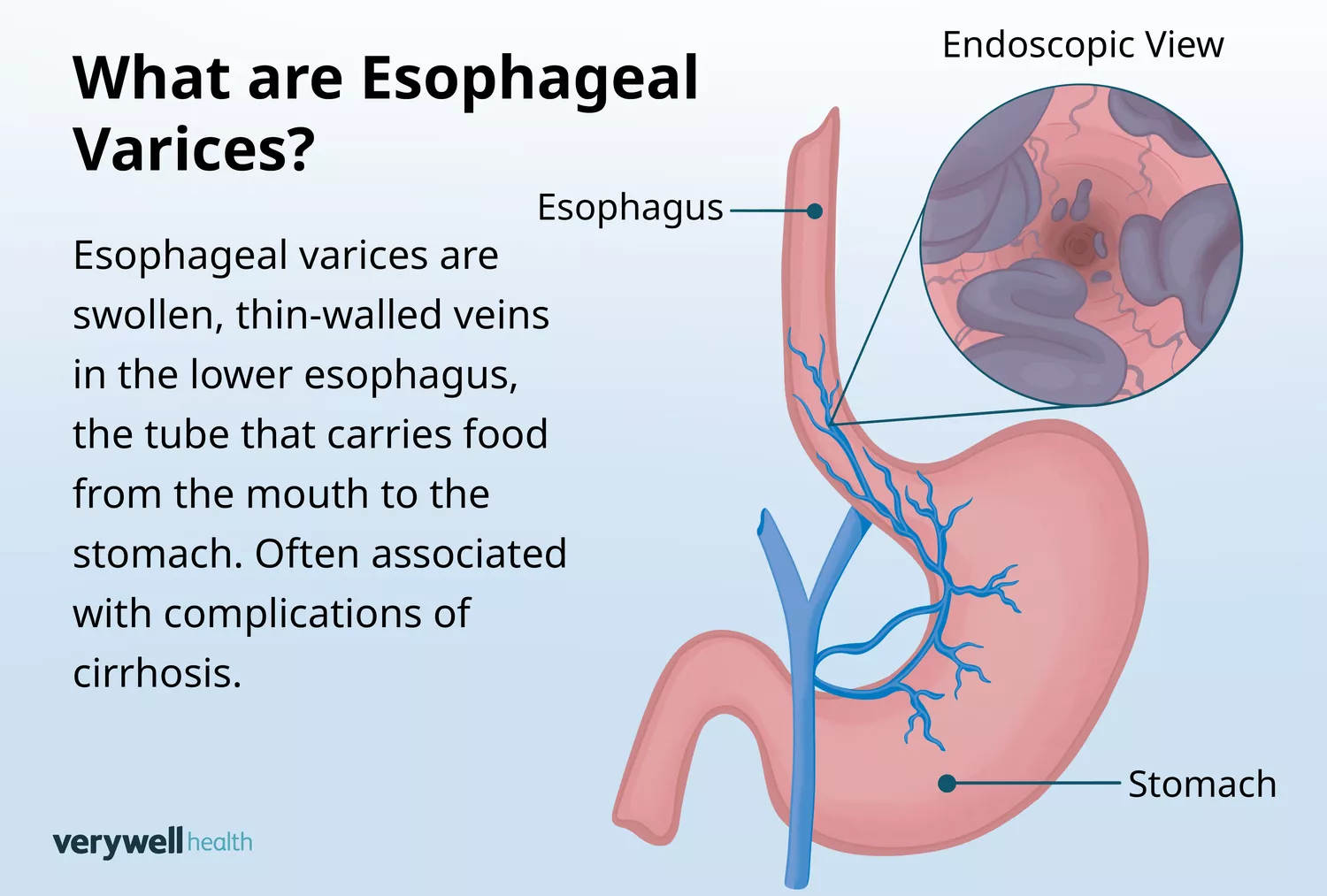
To understand esophageal varices, one must first understand the plumbing of the human liver. Normally, the portal vein carries blood from the digestive organs to the liver for filtering. However, when the liver becomes scarred—a condition known as cirrhosis—the tissue turns stiff and resistant. This creates a "backlog" in the system, significantly raising the pressure within the portal venous system.
While a normal portal pressure sits between 5 and 10 mmHg, portal hypertension risk factors can push this pressure to 15 or 20 mmHg. When the liver cannot handle the volume, the body seeks alternative routes for the blood to return to the heart. It redirects blood into smaller, thinner-walled veins, such as those lining the lower esophagus.
These tiny vessels are not designed to handle high-pressure flow. As they engorge, they become esophageal varices. These veins stretch and thin out, much like an overinflated balloon, making them prone to leaking or catastrophic rupture. Data suggests that in patients with cirrhosis, these veins develop at an annual rate of about 8%. The progression is often tied to the Child-Pugh score, a clinical scale used to assess the prognosis of chronic liver disease. As liver function declines, the pressure in the splanchnic hemodynamics increases, further stressing the gastroesophageal junction.
Recognizing the Signs: From Early Warnings to Rupture
One of the most dangerous aspects of esophageal varices is their silent nature. You cannot feel them growing, and they do not cause pain while they remain intact. However, as portal hypertension worsens, the body may show systemic signs that the liver is struggling. Common indicators include jaundice (yellowing of the eyes and skin), the development of ascites (fluid buildup in the abdomen), and splenomegaly (an enlarged spleen).
When the veins reach a breaking point, the situation shifts from a chronic condition to a medical emergency. Recognizing the signs that esophageal varices have reached a critical stage can be the difference between life and death.
Emergency Triage: The Red Flags of Rupture
If you or someone under your care has a known liver condition, you must be vigilant for these symptoms:
- Hematemesis: This is the most visible sign. It involves vomiting bright red blood or material that looks like coffee grounds.
- Melena: Blood that has passed through the digestive system turns stools black, tarry, and exceptionally foul-smelling.
- Hemodynamic Shock: Significant blood loss leads to sudden dizziness, extreme pale skin, fainting, or a rapid, thready pulse.
Expert Tip: Early warning signs of esophageal variceal bleeding are not always dramatic. Some patients experience a "warning leak" characterized by mild lightheadedness or a sudden drop in energy levels before a major rupture occurs.
If any of these signs appear, emergency first aid for suspected variceal rupture involves keeping the patient calm, lying them on their side to prevent choking on blood, and seeking immediate hospital intervention.
Screening and Risk Assessment
Because the condition is often asymptomatic, clinicians rely on strict esophageal varices screening guidelines for cirrhosis patients. The goal is to catch high-risk veins before they bleed.
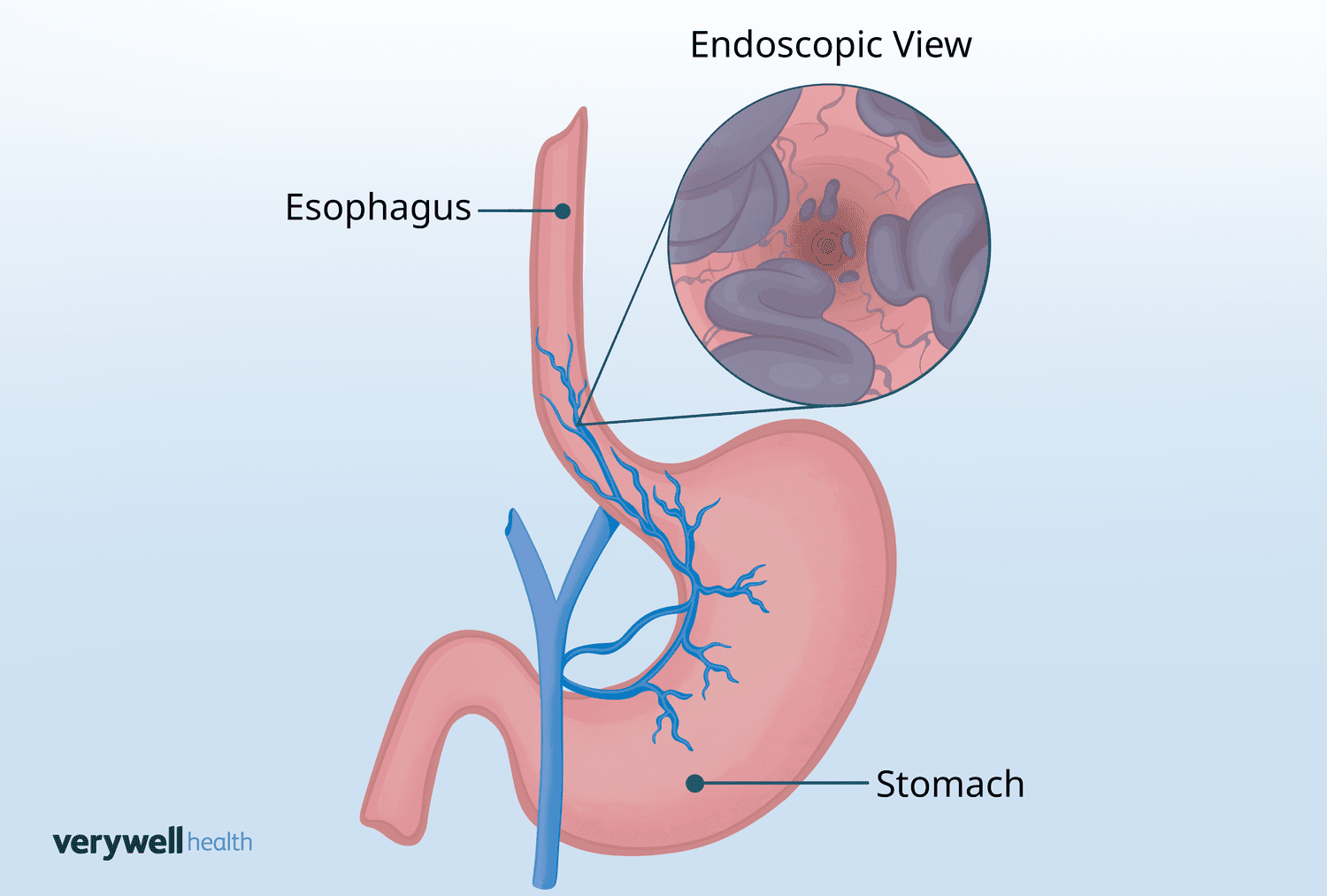
The gold standard for diagnosis is an upper endoscopy (EGD). During this procedure, a doctor inserts a thin camera through the mouth to directly visualize the esophagus. They look for specific "markers" of imminent rupture, such as red wale markings—longitudinal red streaks that look like whip marks on the vein. These markings indicate that the vein wall is dangerously thin.
In addition to endoscopy, modern medicine uses non-invasive tools like FibroScan to measure liver stiffness. A liver stiffness measurement (LSM) higher than 25 kPa often correlates with a higher likelihood of varices. The frequency of screening depends on the stability of the patient:
- Compensated Cirrhosis: Patients with stable liver function and no history of bleeding may only need an endoscopy every 2 to 3 years.
- Decompensated Cirrhosis: Patients with active symptoms like jaundice or ascites usually require yearly evaluations.
The ultimate goal of these screenings is to monitor the hepatic venous pressure gradient. Once the pressure exceeds 12 mmHg, the risk of spontaneous hemorrhage increases exponentially, necessitating a shift from observation to active prevention.
Preventing Variceal Rupture: Medical Strategies
Preventing variceal rupture is divided into two categories: primary prophylaxis (preventing the first bleed) and secondary prophylaxis (preventing a recurrence).
Medication: Lowering the Pressure
The first line of defense often involves non-selective beta-blockers. Unlike standard beta-blockers used for high blood pressure, these medications specifically target the blood flow to the portal vein.
| Medication | Mechanism | Clinical Goal |
|---|---|---|
| Propranolol | Reduces heart rate and constricts splanchnic blood vessels. | Lower portal pressure by roughly 20%. |
| Carvedilol | Combines beta-blocking with alpha-blocking properties to reduce liver resistance. | Often more effective at reaching the <12 mmHg target. |
| Nadolol | A long-acting version of propranolol. | Provides steady, 24-hour pressure management. |
Patients should be aware of medications to avoid with portal hypertension and varices, specifically Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) like ibuprofen or aspirin, as these can increase the risk of bleeding and damage liver function.
Procedural Interventions
For patients who cannot tolerate medications or who have high-risk red wale markings, doctors may perform endoscopic variceal ligation (banding). This involves placing tiny rubber bands around the varices to cut off blood flow, eventually causing them to wither and disappear.
In more severe cases, a Transjugular intrahepatic portosystemic shunt (TIPS) may be necessary. This procedure creates a "bypass" within the liver to relieve the pressure in the portal system. While effective at preventing bleeding, it is usually reserved for those at high risk or those awaiting a liver transplant.
Lifestyle Changes and Long-Term Management
While medical interventions are vital, esophageal varices lifestyle changes play a massive role in long-term survival. The liver has a remarkable capacity for stabilization if the insults to it are removed.
Absolute Alcohol Abstinence This is the most critical step. For patients with alcohol-related cirrhosis, stopping consumption can lead to a significant reduction in portal pressure and even a regression of small varices. Continued drinking is the number one risk factor for a repeat bleeding episode.
Weight and Metabolic Health Obesity-related liver disease (NAFLD/NASH) can worsen portal hypertension. Managing weight through a balanced diet helps reduce the overall burden on the liver. Furthermore, lifestyle changes to prevent esophageal variceal hemorrhage include a low-sodium diet. Excess salt leads to fluid retention and ascites, which in turn increases the pressure within the abdominal cavity and the portal system.
Physical Precautions Patients with large varices should avoid heavy lifting or activities that involve intense "straining" (Valsalva maneuver), as this sudden spike in internal pressure can theoretically trigger a rupture in a very fragile vein.
FAQ
What are the early warning signs of esophageal varices?
Early on, there are usually no symptoms at all. The veins develop silently. However, early signs that they might be bleeding include feeling lightheaded, having a rapid pulse, or noticing that your stools have become darker or black. Systemic signs of the underlying liver disease, such as yellowing of the skin or a swollen abdomen, serve as warning signs that varices may be present.
What is the main cause of esophageal varices?
The primary cause is portal hypertension, which most commonly results from cirrhosis of the liver. When scar tissue blocks the flow of blood through the liver, the blood is forced into smaller veins in the esophagus. Other causes include blood clots in the portal vein or certain parasitic infections that damage the liver.
How long can a person live with esophageal varices?
Life expectancy depends on the stage of the underlying liver disease and whether the varices have ruptured. If caught early through screening and managed with beta-blockers or banding, many people live for decades. However, the six-week mortality rate after a major bleeding event is between 10% and 20%, making prevention the key to longevity.
Can esophageal varices be cured or reversed?
Esophageal varices themselves are a symptom of an underlying problem. While the veins can be removed through banding or their pressure reduced with a TIPS procedure, they are only "cured" if the underlying liver disease is addressed. In cases of early-stage cirrhosis caused by alcohol or Hepatitis C, treating the cause can sometimes lead to the regression of varices.
What happens when esophageal varices burst?
When a varix ruptures, it causes massive internal bleeding into the esophagus and stomach. This leads to vomiting large amounts of blood and a rapid drop in blood pressure. It is a life-threatening medical emergency that requires immediate hospitalization, blood transfusions, and endoscopic treatment to stop the flow.
How are esophageal varices treated?
Treatment focuses on two goals: stopping active bleeding and preventing future episodes. To stop a bleed, doctors use endoscopic banding and medications like octreotide therapy to slow blood flow. To prevent future bleeds, patients are typically prescribed non-selective beta-blockers and scheduled for regular endoscopic check-ups to band any high-risk veins before they burst.





